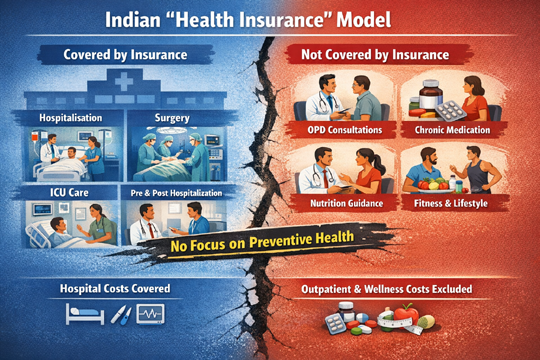
The Indian so-called health insurance model reflects the structural flaws of Indian insurance products. Most policies reimburse inpatient hospital expenses: room charges, surgical procedures, ICU care, and limited pre- and post-hospitalisation costs. Outpatient consultations, long-term medication, nutritional counselling, or exercise programs are either excluded or available through small add-ons with tight caps. Lifestyle orientation for better health is not even considered as health activity
In India, what we commonly call health insurance functions largely as hospitalisation insurance. The distinction is more than linguistic. It shapes incentives, spending patterns, and even how citizens think about illness. A middle-aged professional may pay premiums diligently for a decade, believing he has secured protection for himself and his family. When he is diagnosed with diabetes, however, he discovers that the monthly costs of consultations, laboratory investigations, and medicines—two or three thousand rupees every month—are entirely his responsibility. The insurance policy he has funded for years does not participate in his daily management. Yet if his blood sugar spirals out of control and he lands in an intensive care unit with a bill running into several lakhs, the insurer will pay. The system intervenes at collapse, not at imbalance.
This pattern is not accidental. It reflects the structural design of Indian insurance products. Most policies reimburse inpatient hospital expenses: room charges, surgical procedures, ICU care, and limited pre- and post-hospitalisation costs. Outpatient consultations, long-term medication, nutritional counselling, or exercise programs are either excluded or available through small add-ons with tight caps. The financial architecture therefore shields against sudden, high-cost shocks but ignores predictable, recurring health expenditure. In a country where chronic diseases are rising rapidly, this gap is becoming increasingly visible.
The economic logic behind such design is rooted in how insurance functions. Insurance pools uncertain risks across large populations. It thrives on unpredictability—events that may or may not occur. Chronic diseases such as diabetes or hypertension do not fit neatly into this model. Once diagnosed, they create a near-certain stream of recurring costs. Covering these expenses universally would transform insurance from a risk-sharing mechanism into a routine reimbursement service, requiring significantly higher premiums. Insurers worry that such predictability erodes actuarial balance.
Compounding this challenge is the fragmented nature of outpatient care in India. Much of OPD delivery occurs in small, independent clinics with varying pricing structures and limited digital integration. Billing is not standardised. Records are often not interoperable. Monitoring thousands of small claims of a few hundred rupees each is administratively complex. Fraud perception—whether real or exaggerated—adds another layer of hesitation. Insurers find it easier to audit a single hospital bill of five lakh rupees than to process hundreds of micro-claims of five hundred rupees each.
Yet focusing solely on actuarial prudence overlooks the macroeconomic burden. India spends enormous sums annually on outpatient care, the majority paid out of pocket. For many families, recurring medical costs chip away at savings and create silent financial stress. Moreover, when OPD expenses are not supported, patients may delay routine follow-ups or diagnostic tests, increasing the likelihood of complications that ultimately require hospitalisation. In effect, the system waits for the expensive event it claims to protect against.
There is also a behavioural dimension that cannot be ignored. Chronic diseases are deeply intertwined with lifestyle—dietary habits, physical activity, sleep patterns, stress levels. Medical advice often emphasises prevention, but compliance remains inconsistent. Many patients rely on medication while postponing meaningful lifestyle adjustments. The monthly OPD bill becomes a manageable nuisance. Only when complications become severe does the insured hospitalisation benefit activate. This creates a distorted incentive: financial support aligns with crisis rather than prevention.
If the objective is to build a genuine health-care ecosystem rather than a sick-care financing model, preventive lifestyle integration must move from rhetoric to structure. Insurance cannot remain a passive cheque book for emergencies. It must evolve into a participant in maintaining wellness. That shift requires reimagining both incentives and infrastructure.
One pathway is to embed preventive care into core policy design. Instead of treating wellness as a peripheral rider, insurers could include annual health assessments, nutritional counselling sessions, and structured lifestyle programs as standard benefits. These services would not merely be reimbursable expenses but organised pathways with measurable goals. For example, policyholders with prediabetes could enrol in structured weight management and exercise programs, with digital monitoring to track progress. Insurers could reward documented improvements in health markers—such as reduced HbA1c levels or improved lipid profiles—with premium discounts or wellness credits.
Digital technology makes such monitoring feasible. Wearable devices, teleconsultations, and app-based reporting can provide data on physical activity, sleep, and even dietary compliance. When integrated with secure health records, this information allows insurers to differentiate between active participation and passive neglect. Instead of underwriting only age and medical history, policies could incorporate behavioural metrics. Health becomes a shared responsibility rather than a unilateral payout obligation.
However, preventive ecosystems cannot be built solely through insurance products. The healthcare delivery landscape must also transform. Standardised outpatient networks with transparent pricing and electronic health records would reduce unpredictability. Aggregating small clinics into quality-assured networks could preserve local trust while introducing institutional standards. A hybrid “phygital” approach—combining digital interfaces with physical care—can make preventive consultations accessible and affordable. When routine follow-ups become convenient and affordable, adherence improves.
Community-based initiatives also have a role. Corporate wellness programs, school-based nutrition education, and urban design that encourages physical activity contribute to reducing disease incidence. Insurers and employers could collaborate to co-fund preventive programs, recognising that healthier populations generate fewer claims. Tax incentives for documented participation in wellness programs could further reinforce behavioural alignment.
Traditional systems of medicine, with their emphasis on daily discipline and balanced living, offer philosophical insights into prevention. Concepts of routine, moderation, and seasonal adaptation underscore the idea that health is a continuous practice rather than an episodic repair. Integrating such preventive principles—without descending into unscientific claims—can enrich modern healthcare frameworks. Structured yoga programs, stress management workshops, and dietary education rooted in evidence-based practice could be embedded into wellness benefits.
The policy question remains complex: should insurers be compelled to cover OPD for long-term policyholders? Mandating comprehensive coverage without systemic reform may inflate premiums and reduce affordability. Yet leaving OPD outside the insurance ambit perpetuates the current imbalance. A phased model may offer balance—limited but guaranteed OPD benefits after continuous renewals, combined with mandatory participation in preventive programs for chronic conditions. In such a model, financial support would be linked to engagement in structured care pathways.
Ultimately, the conversation must shift from “Who pays?” to “How do we prevent payment becoming necessary?” The healthcare ecosystem should aim to prevent individuals from becoming long-term patients. This does not imply eliminating disease—a biological impossibility—but reducing preventable progression. When preventive habits are normalised, monitored, and incentivised, the incidence of severe complications declines.
India stands at a pivotal moment in its health transition. Non-communicable diseases are rising, urban lifestyles are increasingly sedentary, and medical technology is expanding rapidly. Continuing with a hospital-centric insurance framework risks escalating costs and widening gaps. Redesigning the system to include preventive lifestyle integration offers an opportunity to align financial incentives with public health goals.
The story of the diabetic policyholder paying monthly out of pocket while holding an unused insurance card symbolises a broader structural contradiction. Financial protection should not activate only at the brink of collapse. A mature health ecosystem would intervene earlier—encouraging discipline, supporting continuity, and rewarding prevention. When insurance evolves from a passive responder to an active partner in wellness, the distinction between hospital insurance and health insurance may finally begin to disappear.